Complications from Medical Tourism
Case Study: Managing Wound Complications After Lumbar Lipectomy and Abdominoplasty
Dr. James R. Benjamin, MD, ASPS & Joyce S. Benjamin, RN, PA-C Emeritus
Background
Body contouring surgeries such as abdominoplasty and lumbar lipectomy inherently involve extensive undermining. This surgical technique creates significant dead space, a setting in which fluid readily accumulates. Cavitating, draining wounds and wound edge dehiscence are recognized complications in these patients.
Negative Pressure Wound Therapy (NPWT), also known as VAC (vacuum-assisted closure), has become a mainstay in managing such complications—reducing wound volume, minimizing dressing frequency, and accelerating closure.
Case Presentation
Patient: P.H., 35-year-old, female, BMI 35
Surgical History: Cesarean section x2, abdominoplasty (2021), back liposuction (later 2021).
In January 2025, the patient traveled to Miami for a lumbar lipectomy. Despite preoperative counseling from a previous surgeon regarding the risks of early travel, she returned home five days post-op.
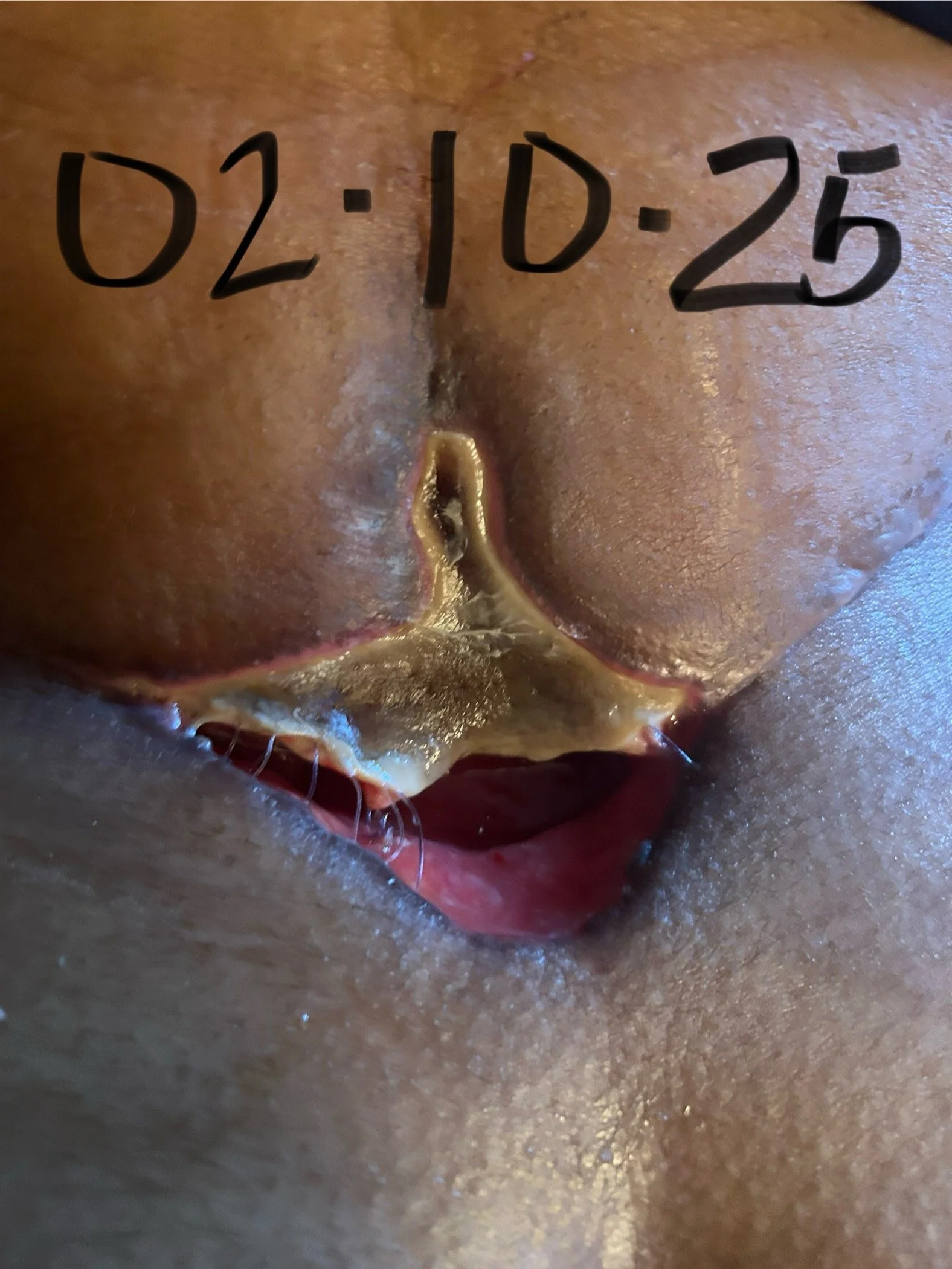
By postoperative day 10, she noted wound edge discoloration progressing to dehiscence with significant drainage. Initial management included wet-to-dry dressings, multiple daily changes, and referral to wound care. Three board-certified plastic surgeons separately evaluated her wound, and each concurred that NPWT would be optimal.
Insurance denied wound vac authorization due to the elective nature of the original cosmetic procedure. Her previous plastic surgeon secured a device independently. Following surgical debridement, NPWT was initiated.
Clinical Course
Before NPWT: Wet-to-dry dressings required multiple daily changes, with little improvement.
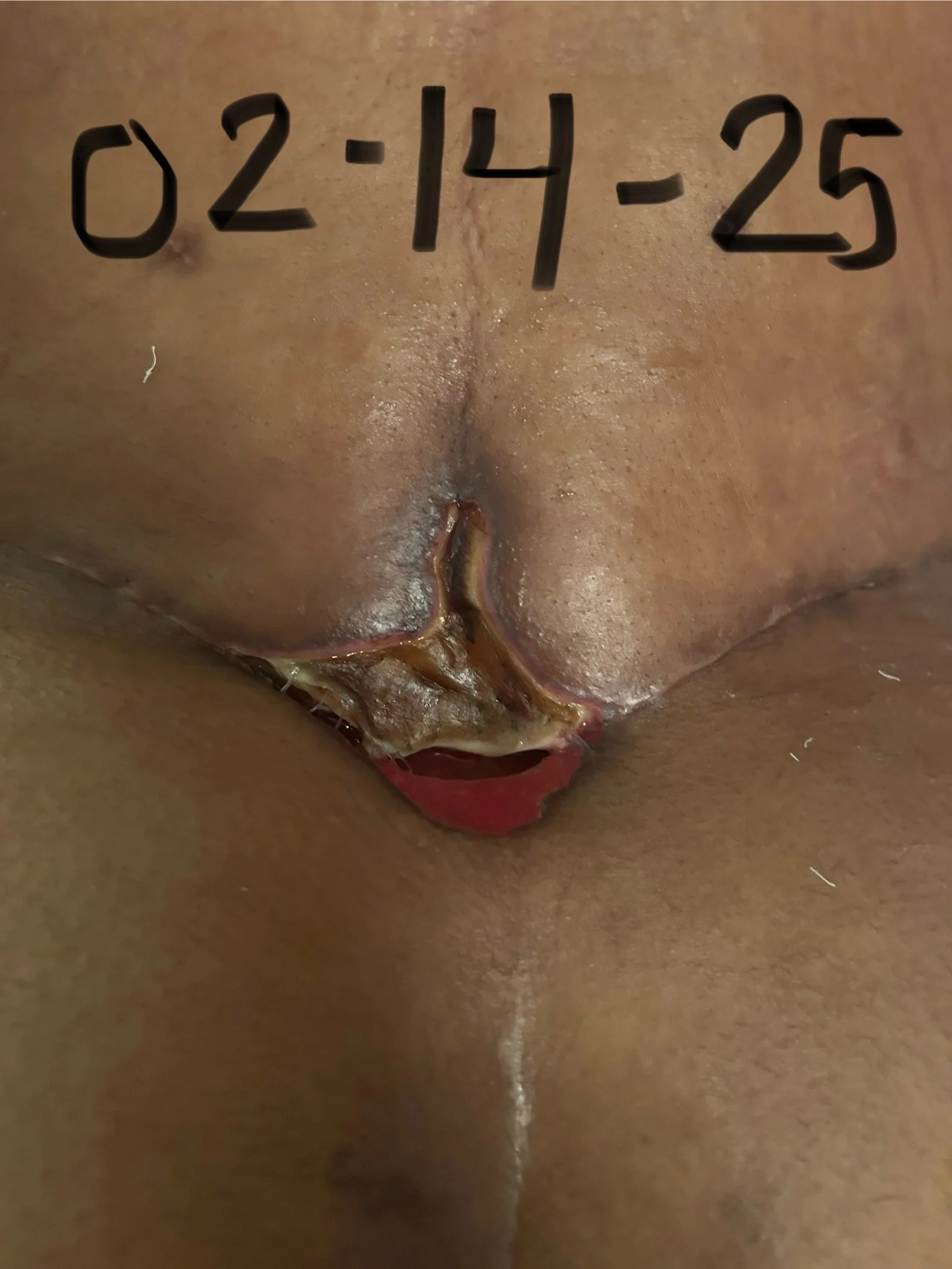
With NPWT: Dressing frequency decreased to every 72 hours. Progressive wound contraction and granulation were documented.
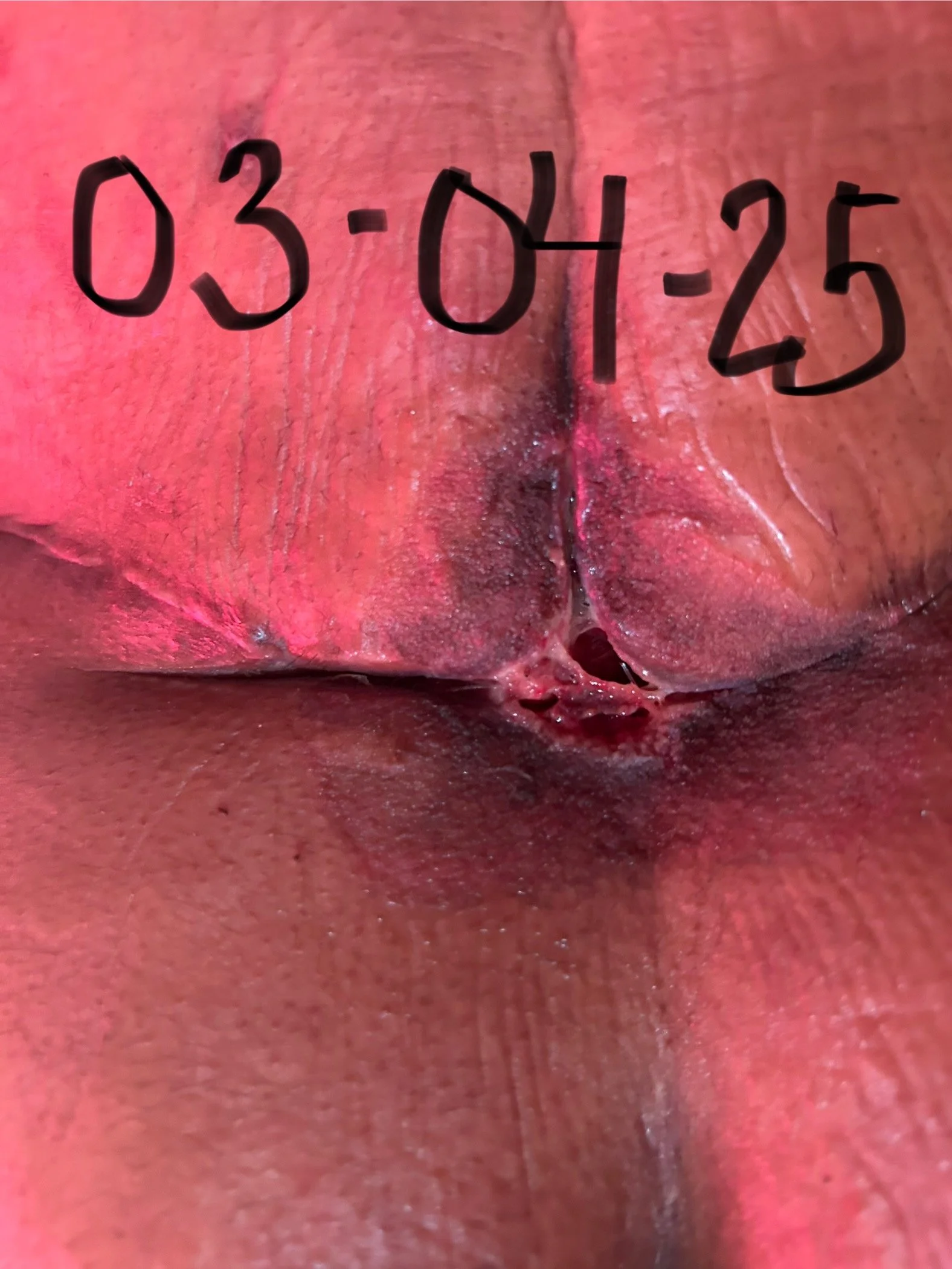
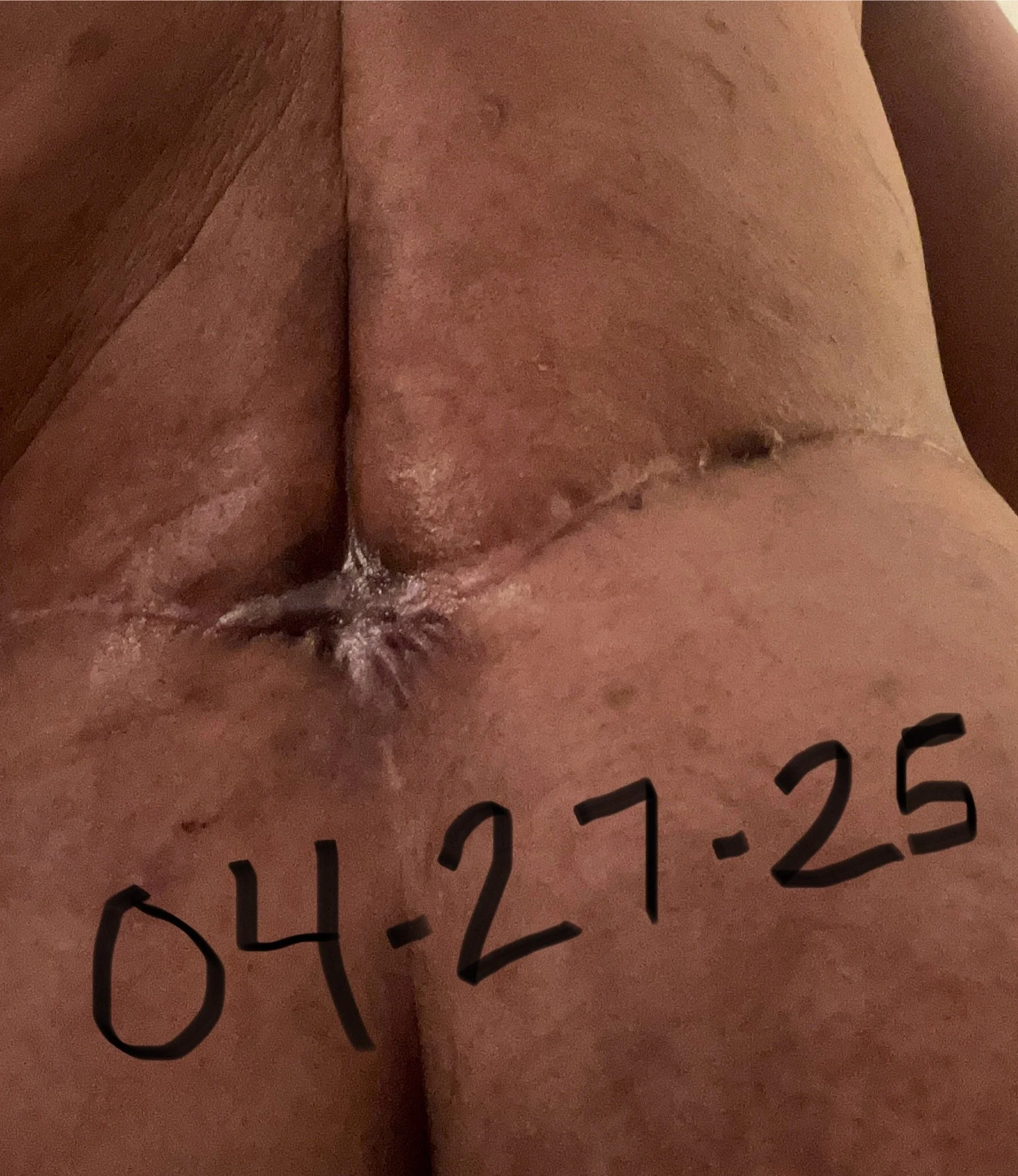
Outcome: By March 25, 2025, wound depth improved from 1.5 cm to 3 mm, with lateral dimensions reduced by nearly half. The wound vac was discontinued, and the wound went on to heal fully by secondary intention by April 12, 2025.











Discussion
This case illustrates several important points:
Travel Restrictions Matter – Early postoperative travel likely contributed to impaired wound healing.
Consensus Among Specialists – Multiple board-certified plastic surgeons independently recommended NPWT, underscoring its value in managing post-contouring dehiscence.
NPWT Efficiency – Dressing burden dropped from several times daily to every three days, while wound healing accelerated.
Barriers of Medical Tourism – Financial and geographic strain complicated access to timely wound management.
Clinical Takeaway – When complications arise, NPWT remains one of the most effective modalities for salvaging surgical outcomes and supporting patients through recovery.
Conclusion
P.H.’s case highlights the dual realities plastic surgeons face: the growing trend of medical tourism in body contouring and the proven efficacy of NPWT in wound complication management. For surgeons, timely recognition and access to NPWT can dramatically alter the trajectory of healing—turning a challenging complication into a successful recovery.